Πρωτοποριακή επέμβαση και στην Ελλάδα για την υπνική άπνοια
Ολοκληρώθηκε με επιτυχία η πρώτη επέμβαση στην Ελλάδα εμφύτευσης γλωσσικού βηματοδότη για την θεραπεία της υπνικής άπνοιας. Απευθύνεται σε ασθενείς με μέτριου και σοβαρού βαθμού υπνική άπνοια, που δεν δέχονται τη θεραπεία με τη μάσκα CPAP.
Η υπνική άπνοια είναι μια διαταραχή στη λειτουργία της αναπνοής κατά τη διάρκεια του ύπνου κατά την οποία ο ασθενής σταματάει να αναπνέει για πάνω από 10 δευτερόλεπτα πολλές φορές κάθε ώρα. Σαν συνέπεια των διακοπών αυτών της αναπνοής, η ποσότητα του οξυγόνου που υπάρχει στο αίμα του ασθενούς μειώνεται με αποτέλεσμα να διαταράσσεται η οξυγόνωση οργάνων όπως ο εγκέφαλος και η καρδιά.
Η πιο συχνά εφαρμοζόμενη θεραπεία για την υπνική άπνοια είναι η θεραπεία με τη μάσκα CPAP. Πολλοί όμως ασθενείς δεν μπορούν να συμμορφωθούν στη χρήση της μάσκας CPAP αφήνοντας την υπνική άπνοια χωρίς θεραπεία.
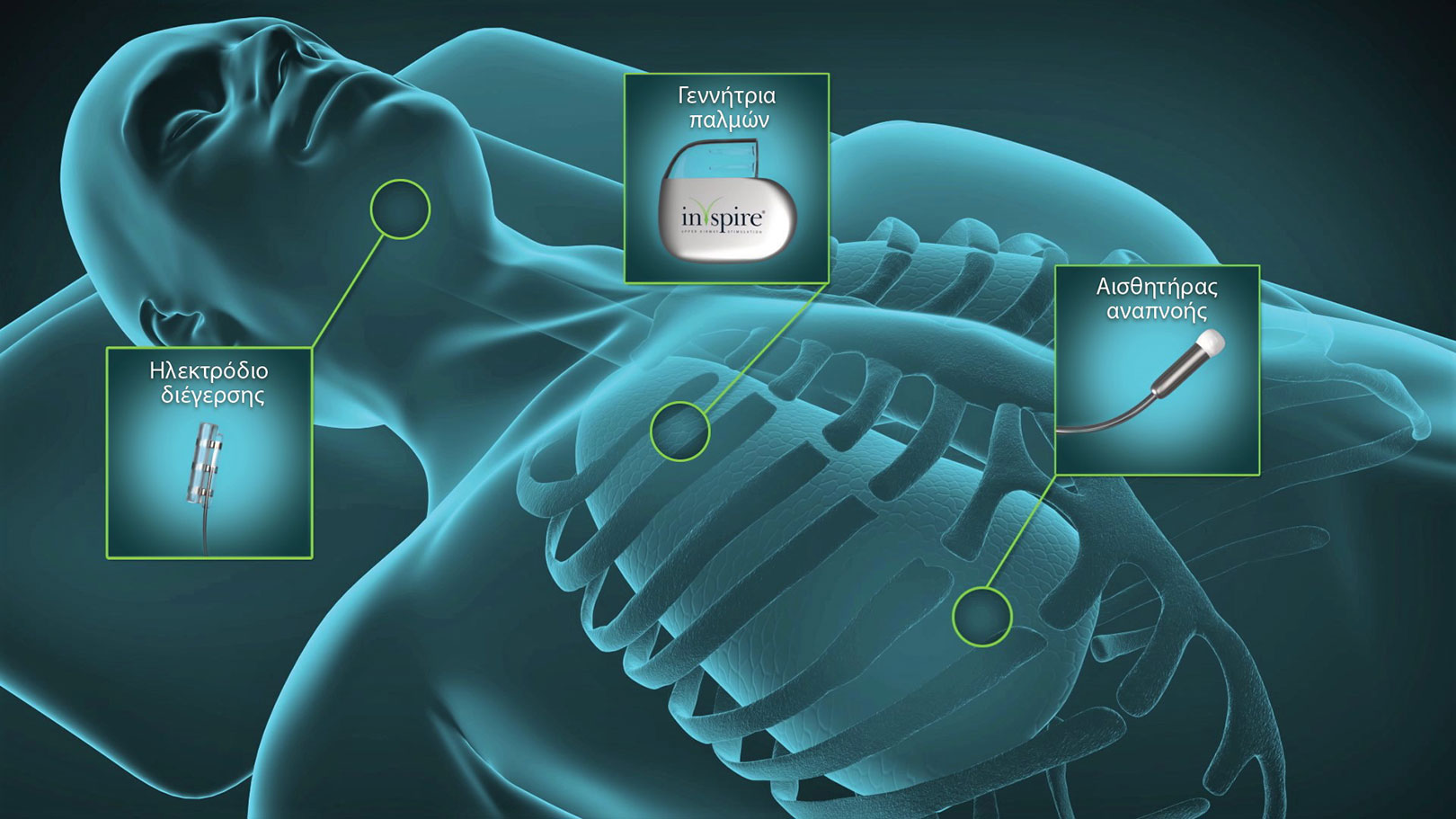
Η νέα μέθοδος αφορά την εμφύτευση ενός γλωσσικού βηματοδότη με το σύστημα Inspire. Η συγχρονισμένη με την αναπνοή απαλή διέγερση του υπογλώσσιου νεύρου διατηρεί τους αεραγωγούς ανοικτούς κατά τη διάρκεια του ύπνου. Μάλιστα, ο ασθενής ελέγχει το σύστημα εύκολα μέσω τηλεχειριστηρίου!
Η θεραπεία είναι εγκεκριμένη από την Αμερικανική Υπηρεσία Τροφίμων και Φαρμάκων (FDA) από το 2014 κι εφαρμόζεται τα τελευταία χρόνια ευρέως στην Αμερική και στην Ευρώπη με πολύ καλά αποτελέσματα. Μέχρι σήμερα, πάνω από 10.000 ασθενείς σε όλο τον κόσμο έχουν ήδη υποβληθεί στη θεραπεία Inspire με επιτυχία.
Σε πολυκεντρική μελέτη στην Γερμανία και στις ΗΠΑ, που περιελάμβανε 508 ασθενείς στους οποίους εμφυτεύτηκε το σύστημα Inspire, ο δείκτης των απνοιών μειώθηκε από 34 σε 7 επεισόδια ανά ώρα ύπνου. Επιπλέον, η 5-ετής παρακολούθηση των ασθενών που έχουν υποβληθεί στη θεραπεία Inspire έχει αποδείξει ότι τα ευεργετικά αποτελέσματα διατηρούνται στο πέρασμα του χρόνου.
Η πρωτοποριακή αυτή επέμβαση πραγματοποιήθηκε για πρώτη φορά στην Ελλάδα από τον χειρουργό ΩΡΛ Ιωάννη Κουτσουρελάκη. Η επέμβαση γίνεται με τρεις μικρές τομές:
- μια τομή στην υπογνάθια χώρα που επιτρέπει την εύρεση του υπογλώσσιου νεύρου και την τοποθέτηση του νευροδιεγέρτη,
- μια τομή στην υποκλείδια χώρα για την τοποθέτηση του βηματοδότη και
- μια τρίτη τομή στο ύψος του 4ου-5ου μεσοπλεύριου διαστήματος για την τοποθέτηση του αισθητήρα ανίχνευσης των αναπνευστικών κινήσεων
Η επέμβαση διήρκησε δύο περίπου ώρες κι ο ασθενής εξήλθε του νοσοκομείου την ίδια ημέρα. Ο Δρ Κουτσουρελάκης έχει συμβάλει στην ανάπτυξη της θεραπείας Inspire από τις πρώτες κιόλας κλινικές δοκιμές και έχει εκπαιδευτεί στο αντικείμενο στην Ολλανδία και στην Αμερική. Είναι ο πρώτος χειρουργός ΩΡΛ πιστοποιημένος για την αντιμετώπιση ασθενών με τη θεραπεία Inspire στην Ελλάδα.
Ο γλωσσικός βηματοδότης δεν θα πρέπει να χρησιμοποιηθεί πριν από την πλήρη επούλωση που γίνεται σε 2 έως 4 εβδομάδες. Περίπου ένα μήνα μετά την εμφύτευση, ακολουθεί η προσαρμογή της θεραπείας στις ανάγκες και τα χαρακτηριστικά του κάθε ασθενή.
Σε αυτό το βήμα, ο ιατρός παρέχει στον ασθενή μια πλήρη εισαγωγή στη λειτουργία του συστήματος Inspire και ενεργοποιεί τη θεραπεία με τις ρυθμίσεις που ταιριάζουν στον ασθενή. Στη συνέχεια, ο ασθενής μπορεί να ενεργοποιήσει τον γλωσσικό βηματοδότη τη νύχτα και να τον απενεργοποιήσει ξανά το πρωί χρησιμοποιώντας ένα τηλεχειριστήριο καθώς και να ρυθμίσει το επίπεδο διέγερσης συνηθίζοντας την νέα θεραπεία.
Οι περισσότεροι ασθενείς χρειάζονται λίγες νύχτες για να συνηθίσουν το σύστημα Inspire και μετά δεν αντιλαμβάνονται καν τη διέγερση. Μετά τη φάση εξοικείωσης διάρκειας περίπου 4 εβδομάδων, ακολουθεί μια μελέτη ύπνου στο εργαστήριο ύπνου όπου οι ρυθμίσεις αναπροσαρμόζονται εάν είναι απαραίτητο.